What is the spinal cord
The spinal cord is the main pathway for information, connecting the brain and peripheral nervous system. It has three major functions: it acts as a conduit for motor information, which travels down the spinal cord; a conduit for sensory information which travels in the reverse direction, and as a center for coordinating certain reflexes.
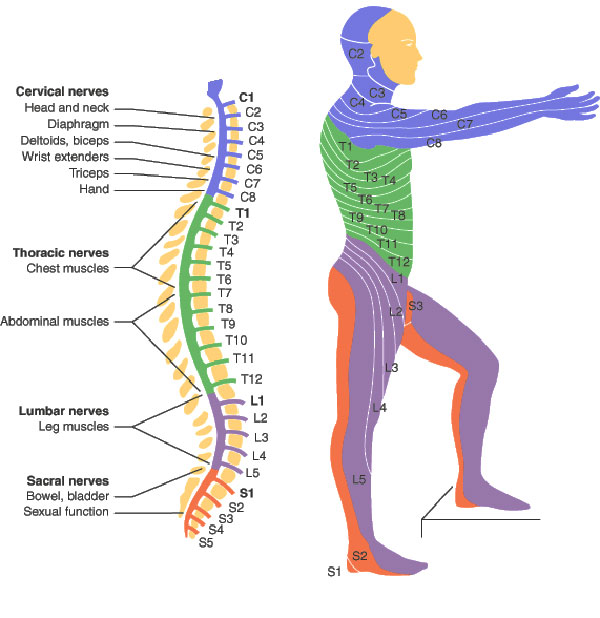
The spinal cord is divided into 31 segments. At every segment, right and left pairs of spinal nerves (mixed sensory and motor) form. In the upper part of the vertebral column, spinal nerves exit directly from the spinal cord, when in the lower part nerves pass further down the column before exiting.
The cervical enlargement, located in C3 – T2 segments, is a level where sensory input comes from and motor output goes to the arms.
The lumbar enlargement, located in L1 – S3 segments, handles sensory input and motor output coming from and going to the legs.
The human brain and spinal cord together form the central nervous system (CNS).
Spinal cord injuries and their consequences
There are two areas of the spinal cord which are most commonly affected by injuries: the cervical spine (C1-C7) and the lumbar spine (L1-L5).
Spinal cord injuries may be caused by trauma to the spinal column (stretching, bruising, applying pressure, severing, laceration, etc.), resulting from a car accident, slip and fall or other types of accident. The vertebral bones or intervertebral disks can shatter, causing the spinal cord to be punctured by sharp fragments of a bone. Usually, spinal cord injuries may result in loss of feeling in certain parts of the body. In case of less severe injuries, an injured person might only suffer loss of hand or foot function. More severe cases may result in paraplegia, quadriplegia or full body paralysis below the segment affected.
Damage to upper motor neuron axons usually results in a characteristic pattern of ipsilateral deficits. These include hyperreflexia, hypertonia and muscle weakness. Lower motor neuronal damage has its own characteristic pattern of deficits. Rather than an entire side of deficits, there is a pattern relating to the myotome affected by the damage. Lower motor neurons are also characterized by muscle weakness, hypotonia, hyporeflexia and muscle atrophy.
Spinal injury may also cause spinal shock or neurogenic shock. Spinal shock is usually a temporary matter, lasting for 24 – 48 hours, and results in a temporary absence of sensory and motor functions. Neurogenic shock lasts longer – for weeks, and can lead to a loss of muscle tone due to disuse of the muscles below the injured segment.
Spinal cord injury levels
Spinal cord injury levels are used to explain the different severities of paralysis, following an injury. Generally, the higher the level of injury to the spinal cord, the greater the degree of paralysis will result.
In order to help understand how the level of spinal cord injury affects a persons mobility, The following spinal cord injury level guide has been produced. This is only a general guide, and because every spinal cord injury is different, there may be variations in functional ability from person to person.
Complete and Incomplete Spinal Cord Injuries
Spinal cord injuries are categorised as two types of injury:
- Complete spinal cord injuries result in no function or sensation below the level of the injury
- Incomplete spinal cord injuries result in some function or sensation below the primary level of the injury
A person with an incomplete injury may be able to move one limb more than another, to feel parts of the body that cannot be moved, or also may have more functioning on one side of the body than the other.
American Spinal Injury Association Impairment Scale (AIS)
AIS is used to help classify differing degrees of spinal cord injury and to compare and understand residual function. It has the following scale values:
A – complete
No motor or sensory function preserved in the lowest sacral segment (S4-S5).
B – sensory incomplete
Sensory function below neurologic level and in S4-S5, no motor function is preserved below neurologic level, and no motor function is preserved more than three levels below the motor level on either side of the body.
C – motor incomplete
Motor function is preserved below neurologic level and more than half of the key muscle groups the single neurological level of injury (NLI) have a muscle grade less than 3.
D – motor incomplete
Motor function is preserved below neurologic level and at least half of the key muscle groups below the single neurological level of injury (NLI) have a muscle grade 3 or greater.
E – normal
Sensory and motor function is normal.
Injuries in different segemts of the spinal cord
Functionality of T10 – L1 Spinal Cord Injury
Mobility and movement
Full head and neck movement with normal muscle strength.
Normal shoulder movement. Full use of arms, wrists and fingers.
Partial paralysis of lower body and legs.
Upper body strength and balance will vary depending on level of injury (the lower the level, the stronger the upper body strength and balance).
A manual wheelchair may be used for everyday living, with an ability to go on uneven surfaces.
Ability to transfer independently from the bed to a chair, and from a chair to a car. It may be possible to transfer from floor to a chair, depending on the person’s upper body strength. It may also be possible to transfer from sitting position to a standing frame independently.
Ability to drive a car adapted with hand controls. Ability to load a wheelchair into the car.
Respiratory system
Normal respiratory system.
Personal care
Should be independent in personal care as long as no other factors are involved (ie, additional injuries, severe spasticity etc.).
Domestic care
Partial domestic assistance, such as heavy household cleaning and home maintenance is required.
Ability to prepare complex meals and perform general household duties independently.
Communication
Normal communication skills apply.
Functionality of C4 Spinal Cord Injury
Mobility and movement
Full head and neck movement, depends on muscle strength.
Limited shoulder movement.
Complete paralysis of body and legs, including finger, wrist or elbow flexion or extension.
Sympathetic nervous system will be compromised, possibility of Autonomic Dysreflexia.
An electric wheelchair may be controlled by either a chin or “sip and puff” controller, this will vary depending on dexterity.
A person with such injuries requires total assistance when transferring from/to a wheelchair. A hoist will have to be used, possibly by two assistants for safety.
Complete assistance required during meals.
Respiratory system
Able to breathe using the diaphragm.
Assistance required to clear secretions from trachea and in coughing.
Personal care
Complete personal assistance is required. The injured person requires assistance with washing, dressing, and with bowel and bladder management.
Domestic care
Complete domestic care, such as household cleaning, washing of clothes and kitchen duties, preparation of meals and general household duties is required.
Communication
May operate a computer using iris recognition, mouth stick or voice recognition. May use a telephone using voice recognition and a headset.
Functionality of C5 Spinal Cord Injury
Mobility and movement
Full head and neck movement with good muscle strength.
Good shoulder movement.
Complete paralysis of body and legs, including finger or wrist movement. No elbow extension, good elbow flexion.
Sympathetic nervous system will be compromised, possibility of Autonomic Dysreflexia.
An electric wheelchair can be controlled with a hand control for uneven surfaces, a manual wheelchair may be used for short distances on flat surfaces.
A person with such injuries requires total assistance when transferring from/to a wheelchair. A hoist will have to be used, possibly by two assistants for safety.
Ability to feed self using feeding strap and fork or spoon during meals. Food will need to be cut.
Ability to drive a car adapted with hand controls. Assistance may be required to load wheelchair into the car.
Respiratory system
Able to breathe using the diaphragm, with low stamina.
Assistance required to clear secretions and in coughing.
Personal care
Complete personal assistance is required. The injured person requires assistance with washing, dressing, and with bowel and bladder management.
Ability to shave and brush hair may be possible with palm straps.
Domestic care
Complete domestic care, such as household cleaning, washing of clothes and kitchen duties, preparation of meals and general household duties is required.
Communication
May operate a computer using a typing stick or voice recognition. May operate a telephone using voice recognition and a headset.
Functionality of C6 Spinal Cord Injury
Mobility and movement
Full head and neck movement with good muscle strength.
Good shoulder movement.
Complete paralysis of body and legs, including finger movement. No elbow extension, no wrist flexion. Good wrist extension, good elbow flexion.
A passive key grip may be present by flexing the wrist backwards, but will be weak.
Sympathetic nervous system will be compromised, possibility of Autonomic Dysreflexia.
An electric wheelchair can be controlled with a hand control for uneven outdoor surfaces, a manual wheelchair may be used for short distances on flat surfaces.
The person will require total assistance when transferring from floor to chair. Assistance will vary for transfer from/to a wheelchair. A sliding board may be used in assisting with the transfer.
Ability to feed self using feeding strap and fork or spoon during meals. Food will need to be cut. Able to make hot drinks with an adapted kettle using a “kettle tipper”.
Ability to drive a car adapted with hand controls. Assistance may be required to load a wheelchair into the car.
Respiratory system
Able to breathe using the diaphragm, with low stamina.
Assistance required to clear secretions and in coughing. Additional coughing techniques can be applied to assist in coughing by leaning forward whilst exhaling.
Personal care
Personal assistance is required. The injured person requires assistance with washing, dressing, and with bowel and bladder management.
Ability to empty own legbag, depending on the person’s dexterity and strength.
Ability to partially dress upper body. Assistance to dress lower body may be required.
Ability to shave, brush hair and brush teeth with palm straps.
Domestic care
Complete domestic care, such as household cleaning, washing of clothes and kitchen duties is required.
Ability to prepare simple meals and perform simple general household duties with adapted equipment.
Communication
May operate a computer using a typing stick or voice recognition. May operate a telephone using voice recognition and a headset.
Functionality of C7 – C8 Spinal Cord Injury
Mobility and movement
Full head and neck movement with good muscle strength.
Good shoulder movement.
Complete paralysis of body and legs.
Partial finger movement, full elbow extension and flexion, full wrist extension and flexion.
A person with a C7 injury will have movement in the thumb.
Sympathetic nervous system will be compromised, possibility of Autonomic Dysreflexia.
May use an electric wheelchair for long independent travel or on uneven outdoor surfaces. A manual wheelchair may be used for short distances on flat surfaces.
Ability to transfer independently from the bed to a chair, and from a chair to a car. Car transfers may require assistance, depending on the person’s upper body strength.
Ability to drive a car adapted with hand controls. Assistance may be required to load a wheelchair into the car.
Ability to feed self independently during meals. Food may need to be cut. Able to make hot drinks, may require an adapted kettle using a “kettle tipper”.
Respiratory system
Able to breathe using the diaphragm, with low stamina.
Assistance required to clear secretions and in coughing. Additional coughing techniques can be applied to assist in coughing by leaning forward whilst exhaling.
Personal care
Ability to manage bladder and bowel independently will vary depending on the person’s strength and dexterity.
Independent in upper body showering and dressing. Lower body dressing and showering may need assistance.
Independent in grooming, usually without palm straps.
Domestic care
Partial domestic assistance, such as heavy household cleaning, home maintenance, and complex preparation of meals is required.
Ability to prepare simple meals and perform simple general household duties independently.
Communication
May operate a computer using a typing stick or voice recognition. May operate a telephone using voice recognition and a headset.
Functionality of T1 – T4 Paraplegic
Mobility and movement
Full head and neck movement with normal muscle strength.
Normal shoulder movement. Full use of arms, wrists and fingers.
Complete paralysis of lower body and legs.
Upper body strength will vary depending on level of injury (the lower the level, the stronger the upper body strength and balance).
A person with a T4 injury will have good strength in the chest muscles (progressively weaker the higher up the injury is).
Sympathetic nervous system may be compromised, possibility of Autonomic Dysreflexia.
May use an electric wheelchair for long distance independent travel or on uneven outdoor surfaces. A manual wheelchair may be used for everyday living, with an ability to go on uneven surfaces for short distances.
Ability to transfer independently from the bed to a chair, and from a chair to a car. Car transfers may need assistance, depending on the person’s upper body strength.
Ability to drive a car adapted with hand controls. Assistance may be required to load a wheelchair into the car.
Ability to feed self independently during meals.
Respiratory system
Ability to breathe normal. Respiration capacity and endurance may be compromised.
Personal care
Should be independent in personal care as long as no other factors are involved (ie, additional injuries, severe spasticity etc.).
Domestic care
Partial domestic assistance, such as heavy household cleaning and home maintenance is required.
Ability to prepare complex meals and perform general household duties independently.
Communication
Normal communication skills apply.
Functionality of T5 – T9 Spinal Cord Injury
Mobility and movement
Full head and neck movement with normal muscle strength.
Normal shoulder movement. Full use of arms, wrists and fingers.
Complete paralysis of lower body and legs.
Upper body strength will vary depending on level of injury (the lower the level, the stronger the upper body strength and balance).
A manual wheelchair may be used for everyday living, with an ability to go on uneven surfaces.
Ability to transfer independently from the bed to a chair, and from a chair to a car. Car transfers may need assistance, depending on the person’s upper body strength.
Ability to drive a car adapted with hand controls. Assistance may be required to load a wheelchair into the car.
Respiratory system
Ability to breathe normal. Respiration capacity and endurance may be compromised.
Personal care
Should be independent in personal care as long as no other factors are involved (ie, additional injuries, severe spasticity etc.).
Domestic care
Partial domestic assistance, such as heavy household cleaning and home maintenance is required.
Ability to prepare complex meals and perform general household duties independently.
Communication
Normal communication skills apply.
Functionality of T10 – L1 Spinal Cord Injury
Mobility and movement
Full head and neck movement with normal muscle strength.
Normal shoulder movement. Full use of arms, wrists and fingers.
Partial paralysis of lower body and legs.
Upper body strength and balance will vary depending on level of injury (the lower the level, the stronger the upper body strength and balance).
A manual wheelchair may be used for everyday living, with an ability to go on uneven surfaces.
Ability to transfer independently from the bed to a chair, and from a chair to a car. It may be possible to transfer from floor to a chair, depending on the person’s upper body strength. It may also be possible to transfer from sitting position to a standing frame independently.
Ability to drive a car adapted with hand controls. Ability to load a wheelchair into the car.
Respiratory system
Normal respiratory system.
Personal care
Should be independent in personal care as long as no other factors are involved (ie, additional injuries, severe spasticity etc.).
Domestic care
Partial domestic assistance, such as heavy household cleaning and home maintenance is required.
Ability to prepare complex meals and perform general household duties independently.
Communication
Normal communication skills apply.
Functionality of L2 – S5 Spinal Cord Injury
Mobility and movement
Full head and neck movement with normal muscle strength.
Normal shoulder movement. Full use of arms, wrists and fingers.
Full upper body control and balance.
Some hip, knee and foot movement depending on the level of injury (the lower the injury, the more control over movement).
A manual wheelchair may be used for everyday living, with an ability to go on uneven surfaces.
Ability to transfer independently from the bed to a chair, and from a chair to a car. It may be possible to transfer from floor to a chair, depending on the person’s upper body strength.
Slow and difficult walking may be possible with assistance or aids (depends on the level of injury).
Ability to drive a car adapted with hand controls. Ability to load a wheelchair into the car.
Respiratory system
Normal respiratory system.
Personal care
Should be independent in personal care as long as no other factors are involved (ie, additional injuries, severe spasticity etc.).
Domestic care
Partial domestic assistance, such as heavy household cleaning, home maintenance is required.
Ability to prepare complex meals and perform general household duties independently.
Communication
Normal communication skills apply.